GLP 1 Guide: Master Weight Loss & New Habits

GLP-1s have moved from niche diabetes medications to a major part of the weight care conversation. In the US, prescriptions for GLP-1 receptor agonists surged 587% from 2019 to 2024, and among adults without a type 2 diabetes diagnosis, prescriptions rose nearly 1,961% for weight management use, according to HealthVerity’s review of FAIR Health data.
That kind of growth explains why so many people feel both curious and confused. You hear names like Ozempic, Wegovy, Zepbound, and Mounjaro everywhere. What often gets lost is the practical question: how do these medications fit into real life, especially if you want changes that last?
A good glp 1 guide shouldn't treat the medication like magic. It should help you understand what the drug is doing, what it isn't doing, and how to use the quieter hunger signals as a chance to build steadier eating habits, better body awareness, and less reactive decision-making around food.
The Rise of GLP-1s What You Need to Know
The speed of change matters here. GLP-1s didn't just become popular. They changed the way many patients and clinicians think about obesity treatment.
For years, many people were told to rely on willpower, stricter dieting, or more exercise alone. The recent prescription surge suggests a different view is taking hold. Weight regulation isn't just about discipline. Biology plays a major role in hunger, fullness, cravings, and how hard it feels to stay consistent.
Why so many people are paying attention
These medications are getting attention because they can change the day-to-day experience of eating. People often describe less “food noise,” fewer constant thoughts about snacks, and an easier time stopping when they feel satisfied.
That doesn't mean every person has the same experience. It also doesn't mean medication replaces skill-building. It means the internal environment may become calmer, and that calm can make behavior change more realistic.
Big shift: GLP-1s are changing obesity care because they address appetite regulation, not just calorie math.
What this means for a beginner
If you're new to this topic, start with three ideas:
- These are medical therapies: Drugs like Wegovy, Ozempic, and Zepbound affect real body systems tied to blood sugar, digestion, and appetite.
- Weight loss is only one part of the story: Many people also care about steadier energy, fewer binge-restrict cycles, and feeling more in control around food.
- Comparisons can get confusing fast: If you're sorting through newer drug classes and how they differ, this explainer on Tirzepatide vs Retatrutide can help clarify the conversation.
The most useful mindset is to treat a GLP-1 like a tool. Not a shortcut. Not a failure. Not a lifetime sentence either. For many people, it's more like temporary scaffolding that can make it easier to build habits that were much harder to practice in a louder, hungrier body.
How GLP-1s Rewire Your Body's Signals
GLP-1 medications can feel mysterious until you think of your body as a communication network. Your gut, pancreas, liver, stomach, and brain are constantly sending messages about hunger and blood sugar. A GLP-1 changes the clarity and timing of those messages.
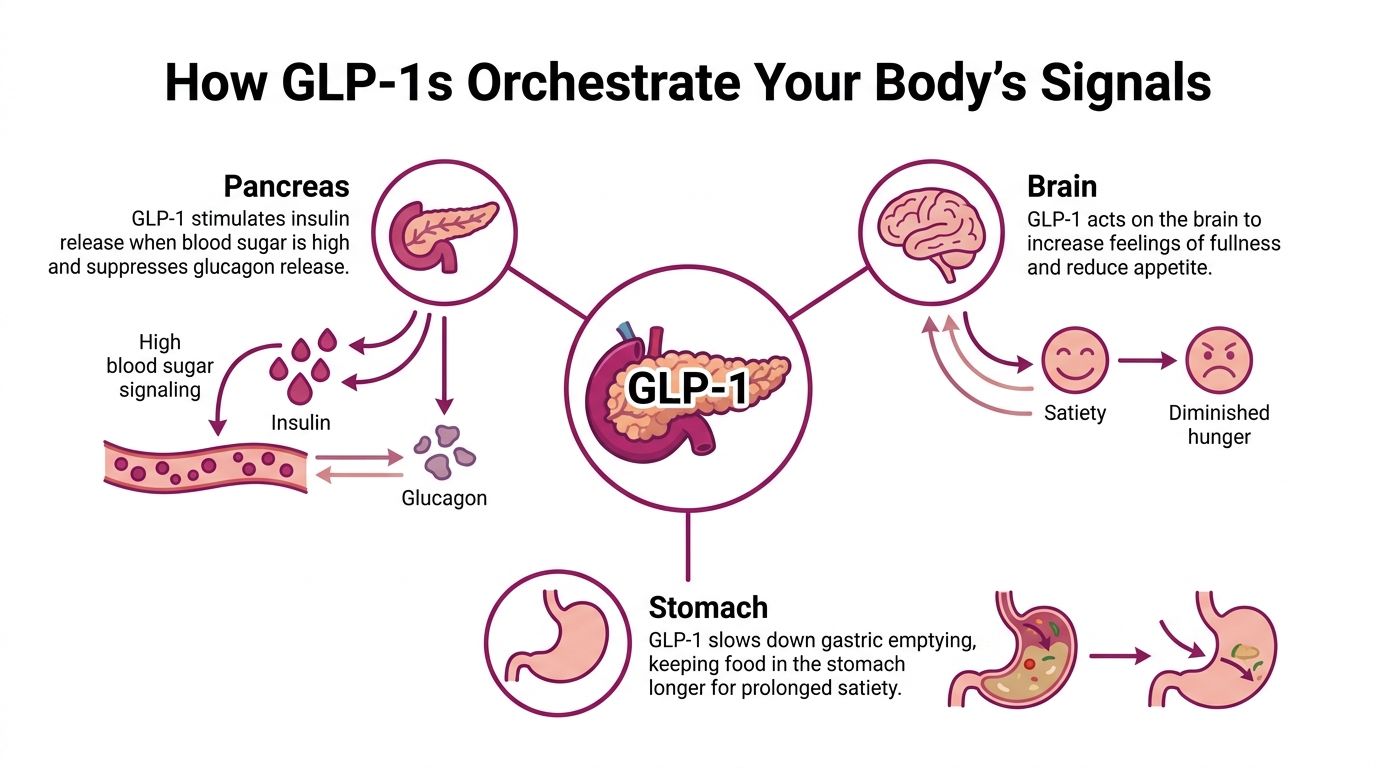
One helpful way to think about it is this: the medication doesn't “force” weight loss. It helps your internal signals act less chaotically. According to Endocrinology Advisor’s GLP-1 overview, GLP-1s work in three main ways: they enhance insulin secretion only when blood sugar is high, suppress glucagon to reduce sugar production by the liver, and delay gastric emptying, which promotes fullness.
The pancreas and liver effect
Your pancreas helps manage blood sugar. GLP-1s act a bit like a smarter thermostat.
When blood sugar rises, the medication helps the pancreas release insulin. At the same time, it suppresses glucagon, a hormone that tells the liver to release more sugar into the bloodstream. The result is a steadier glucose response.
In real life, that can matter because blood sugar swings often affect energy, cravings, and how urgent hunger feels. A more stable pattern doesn't solve every eating struggle, but it can lower the background chaos.
The stomach effect
GLP-1s also slow gastric emptying. That's the process of food moving out of the stomach.
A simple analogy is a traffic controller at a busy intersection. Instead of meals rushing through quickly, digestion slows down. Food stays in the stomach longer, and fullness tends to last longer too.
That helps explain why someone on a GLP-1 may look at a meal they used to finish easily and realize halfway through, “I'm done.” It isn't always about trying harder. The signal arrives earlier.
A visual summary can make this easier to grasp:
The brain effect
The third piece is the brain. GLP-1s act on areas involved in appetite and satiety.
Readers often get confused about this. Fullness isn't just a stomach feeling. It's also a brain interpretation. Your brain decides whether you've had enough, whether food still seems rewarding, and whether hunger feels calm or demanding.
A GLP-1 doesn't just affect your stomach. It changes how your brain reads hunger and satisfaction.
That shift is why many people report less grazing, fewer intrusive food thoughts, or less urgency around emotional triggers. The medication doesn't erase habits or feelings. It can lower the volume so you can hear your own choices more clearly.
Why this matters for habit formation
If your hunger cues have felt unreliable for years, this can be a relief. But it's also an opening.
When appetite quiets down, you get a chance to practice new skills:
- Pausing before eating: Ask whether you're physically hungry, emotionally activated, or just on autopilot.
- Stopping earlier: Learn what comfortable fullness feels like before discomfort.
- Choosing more intentionally: Use the quieter hunger to build meals that support energy and satiety.
That's why a glp 1 guide should always connect the biology to behavior. The medication may calm the signal. You still build the routine.
Expected Results for Weight Loss and Metabolic Health
A common question is simple: what kind of weight loss is realistic?
Clinical trials show meaningful results, but context matters. Trial outcomes reflect structured settings, close follow-up, and consistent dosing. Real life is messier. Still, trial data give a useful benchmark for what's possible.
According to this prescriber guide on GLP-1 receptor agonists, tirzepatide in the SURMOUNT-1 trial led to average weight loss of up to 22.5% at the highest dose, while semaglutide showed around 15% loss in its key trials. The same source notes that 89% to 91% of participants on the highest doses lost at least 5% of body weight.
What those results mean in plain language
A loss of 5% of body weight is often considered clinically meaningful. It can support improvements in health markers and daily functioning. Many people on these medications go beyond that threshold.
The bigger lesson is that GLP-1s and dual-action medications like tirzepatide don't just create tiny changes. For many patients, they create enough appetite shift to change eating patterns in a noticeable way.
But higher average weight loss doesn't mean one medication is “right” for everyone. Tolerability, medical history, coverage, availability, and personal preferences all matter.
GLP-1 medication comparison
| Feature | Wegovy (semaglutide) | Zepbound (tirzepatide) |
|---|---|---|
| Drug type | GLP-1 receptor agonist | Dual GIP/GLP-1 agonist |
| Weight loss in major obesity trials | Around 15% | Up to 22.5% |
| Share losing at least 5% on highest doses | Included in the reported 89% to 91% range | Included in the reported 89% to 91% range |
| What patients may notice | Reduced appetite, earlier fullness | Reduced appetite, earlier fullness, often stronger weight-loss effect in trials |
Trial averages help set expectations, but your lived result depends on consistency, side effects, dose progression, and the habits you build alongside treatment.
Success isn't only the number on the scale
People often focus only on pounds lost. That's understandable, but it's incomplete.
Metabolic health also includes things like blood sugar regulation, appetite control, and a steadier relationship with meals. Sometimes the first win isn't dramatic weight change. It's noticing that you're no longer bargaining with cravings all afternoon, or that dinner doesn't turn into a nighttime spiral.
If you're comparing brand names and trying to sort through how clinicians frame the differences, Mounjaro vs Ozempic for Weight Loss is a practical side-by-side resource.
Navigating Common Side Effects and Safety
The most common side effects with GLP-1s are digestive. That's not surprising, because one of the medication's core actions is slowing digestion.
Nausea is the side effect people mention most often. In trials of semaglutide, nausea affected up to 44% of users on the maintenance dose, compared with 17% on placebo. Most gastrointestinal side effects were mild to moderate and tended to decrease over time. That pattern was noted in the source cited earlier on GLP-1 mechanisms.
What side effects often feel like
People don't all experience the same symptoms, but common early complaints include:
- Nausea after meals: Often worse with large portions or rich foods.
- Early fullness: You may feel done eating much sooner than expected.
- Constipation or diarrhea: Slower digestion can change bowel patterns.
- Food aversion: Some foods may suddenly feel too heavy or unappealing.
This is one reason dose increases are gradual. Your body usually needs time to adapt.
Practical ways to make side effects easier
A few simple adjustments can help a lot:
- Eat smaller meals: A large plate can feel overwhelming when stomach emptying is slower.
- Go gently with fatty foods: Greasy or very rich meals often intensify nausea.
- Slow down at meals: It takes time to notice the new fullness signal.
- Sip fluids regularly: Hydration matters, especially if you're eating less or dealing with GI symptoms.
- Stop before discomfort: “Satisfied” is the target, not stuffed.
Practical rule: If a food suddenly feels hard to tolerate, don't force it just because it used to fit your plan. Work with what's manageable and build back gradually.
What about serious risks
Balance matters here. You want to be informed without spiraling.
Some warnings and precautions require a medical discussion, especially if you have a personal or family history that affects medication choice. That's why these drugs belong in a clinician-guided plan. If side effects are severe, persistent, or escalating, your prescriber needs to know.
The goal isn't to “push through” everything. The goal is to find out whether your dose, pace, meal structure, or medication choice needs adjustment.
Pairing GLP-1s with Sustainable Habits
Long-term success rarely comes from medication alone. It comes from what you practice while the medication is making appetite and fullness easier to hear.
A helpful way to understand GLP-1 treatment is as scaffolding. Scaffolding supports a building while the underlying structure is being strengthened. In the same way, a GLP-1 can support you while you build steadier habits around meals, cravings, stress, and self-awareness. That framing matters for one big reason. Many people worry, understandably, that the weight will come back if the medication changes or stops.
As noted earlier in the article, emerging guidance encourages pairing GLP-1 therapy with psychology-based behavior support, so the work includes more than appetite reduction alone.
Use the quieter appetite to practice new patterns
When hunger gets quieter, you get a rare practice window. The old urgency around food may soften enough for you to notice what is habit, what is stress, and what is true physical need.
That does not mean eating as little as possible. It means learning how to feed yourself on purpose.
A practical approach looks like this:
- Build meals with staying power: Start with protein, add fiber-rich foods you tolerate well, and include enough food to keep meals from turning into accidental under-eating.
- Pause halfway through: Ask, “Am I still physically hungry, or am I eating because the meal is in front of me?”
- Notice repeated situations: Look for patterns such as work stress, late-night fatigue, social pressure, or boredom after dinner.
These small pauses teach a skill many adults have never had a fair chance to build. You begin separating appetite, habit, emotion, and environment instead of experiencing them as one blur.
Emotional eating may get clearer, not disappear
If food has been comfort, reward, distraction, or relief, medication may lower the physical drive to eat without changing the emotional cue that starts the pattern.
That can feel unsettling at first.
You may still want the snack during an argument. You may still crave takeout after a draining day because it signals comfort and a break from decision-making. The difference is that the food may no longer deliver the same emotional payoff. That gap can teach you a lot, if you pay attention to it.
You might notice:
- reaching for snacks during conflict without much physical hunger
- wanting a treat after a hard day because it marks the transition out of stress
- missing the ritual of eating as a way to unwind
Habit work begins in those moments.
A quieter appetite can make emotional patterns easier to see. That visibility gives you something concrete to work with.
Protect muscle, energy, and consistency
Lower appetite can make it easy to under-eat without meaning to. Over time, that can chip away at energy, strength, and the ability to stay consistent with daily life.
Your body still needs regular fuel. A useful GLP-1 guide connects the biology to behavior, because eating well on these medications is not only about less hunger. It is also about preserving muscle, covering basic nutrition, and keeping routines stable enough to last.
A few anchor habits help:
- Keep a short protein list: Know which foods feel manageable when appetite is low.
- Do regular strength work: Resistance exercise gives your body a reason to keep lean tissue.
- Use meal reminders if needed: Some people get so disconnected from hunger cues that they forget to eat until they feel weak.
- Adjust food texture and size: If big salads, heavy meals, or certain vegetables feel rough, switch to gentler options and smaller portions.
Build habits that can outlast the prescription
Fear of weight regain is common, and it makes sense. The answer is not hoping your body will somehow remember what to do later. The answer is practicing repeatable behaviors now, while the medication is lowering the volume on hunger and food noise.
That might mean:
- keeping a simple breakfast routine that feels easy to tolerate
- taking a short walk after a meal that already fits your day
- writing down cravings and what was happening emotionally when they showed up
- doing a one-minute check-in after lunch about hunger, fullness, and satisfaction
Superbloom is one example of a tool designed for that kind of pattern-tracking, with daily check-ins, meal feedback, and reflection prompts focused on habits and emotional triggers rather than calorie counting.
The goal is bigger than short-term appetite control. You are using a period of medical support to rehearse the skills of long-term self-care.
Partnering with Your Clinician for Success
The best outcomes usually come from collaboration, not passive prescribing. Bring questions. Bring observations. Bring the messy details of real life.
A GLP-1 plan works better when your clinician understands how you eat, what side effects you're noticing, what success means to you, and what obstacles could get in the way.
Questions worth bringing to your appointment
Before starting, ask:
- What is this medication meant to help with for me personally? Weight, blood sugar, appetite control, or several things at once?
- How will we decide whether it's working? Ask about markers beyond the scale, such as eating patterns, energy, or metabolic goals.
- What side effects should I expect early on? Ask what is common versus what needs a call right away.
During treatment, ask:
- How should I handle dose increases if symptoms are rough?
- What should I do if I'm barely hungry and start skipping meals?
- Should I adjust how I exercise or structure meals while taking this?
If you're thinking ahead, ask:
- What's our plan if I need to stop, pause, or switch medications?
- How can I reduce the chance of regaining weight if treatment changes?
- Would extra support from a dietitian, therapist, or coach make sense for me?
What to track between visits
You don't need a perfect spreadsheet. A few notes can make appointments much more productive.
Track things like:
- hunger changes
- side effects and when they happen
- foods that feel easier or harder to tolerate
- emotional eating episodes
- energy, strength, and meal regularity
That kind of detail helps your clinician make better decisions than “I think it's going okay.”
GLP-1 FAQ Addressing Common Myths
Will I gain all the weight back if I stop?
Weight regain can happen. The bigger predictor is whether you used the period of lower hunger to build repeatable skills.
A GLP-1 works like a scaffold around a building under repair. The scaffold supports the work for a while. The lasting result comes from what gets built during that time. In real life, that means regular meals, enough protein, noticing early fullness, and having a plan for stress, boredom, or loneliness that does not depend only on food.
That is why many people do best when they treat the medication as support for practice, not as the whole plan.
Are GLP-1s a shortcut?
GLP-1s are medical treatment for biology that may have been pushing appetite, blood sugar, and food noise in the wrong direction for years.
The “shortcut” label misses what patients feel. For many people, the change is less about effortless weight loss and more about finally having enough quiet in their system to pause, choose a meal, and notice when they are satisfied. That pause matters. It gives you a chance to build habits on steadier ground.
Medication can lower the volume of hunger. You still need skills for shopping, meal rhythm, emotional eating, sleep, and movement.
What if I can't afford one?
Cost blocks access for many people, and coverage rules can be confusing. A useful next step is to ask your clinician's office specific insurance questions and get the answers in writing when possible.
You can ask:
- whether your plan covers obesity treatment, diabetes treatment, or neither
- whether prior authorization is required
- whether there are covered alternatives
- whether documentation of related health conditions changes access
Vida explains some of the barriers patients can run into, including coverage gaps and inequities in care, in its review of GLP-1 access barriers.
Do I still need to care about habits if the medication is working?
Yes.
In fact, habits often matter more once the medication starts helping, because you can practice eating and coping with less internal resistance. That is the moment to build a pattern you can keep. A steadier breakfast. A simple lunch you tolerate well. A pause before stress eating. A bedtime routine that protects sleep and next-day appetite.
Those small reps are how temporary medical support turns into longer-term stability.
If you're using a GLP-1 or considering one, Superbloom can help you turn quieter hunger into lasting habits through daily reflection, meal feedback, and support for stress and emotional eating without strict diets or calorie counting.